INTRODUCTION
- DDH ranges from mild acetabular dysplasia with a stable hip through more severe forms of dysplasia, often associated with neonatal hip instability, to established hip dysplasia with/without later subluxation or dislocation
- Delayed diagnosis requires more complex treatment and has a less successful outcome than dysplasia diagnosed early
- Screening for DDH is part of the newborn and infant physical examination (NIPE)
MORE COMMON IN BABIES WITH
- Family history of first degree relative with DDH
- Breech presentation during pregnancy
- Hip abnormality on clinical examination
- Structural foot abnormality – congenital calcaneovalgus, fixed talipes equinovarus
- Significant intrauterine moulding – congenital torticollis, congenital plagiocephaly
- Birth weight >5 kg
- Oligohydramnios
- Multiple pregnancy
- Prematurity
- Neuromuscular disorders
SCREENING FOR DDH
- All babies are offered a NIPE to be completed by aged 72 hr, to include:
- questions to the parents to identify risk factors for DDH and a thorough examination for hip abnormalities
- ask parents: “Is there anyone in the baby’s close family, i.e. mother, father, brother or sister, who has had a hip problem that started when they were a baby or young child and that needed treatment with a splint, harness or operation?”
- Ortolani and Barlow tests, to detect an unstable hip, or hip that is dislocated or subluxed but reducible
- will not detect an irreducible hip, which is best detected by identifying limited abduction of the flexed hip
- questions to the parents to identify risk factors for DDH and a thorough examination for hip abnormalities
HIP EXAMINATION
Observe for
- Symmetry of leg length
- Level of knees when hips and knees are both flexed
Manipulation
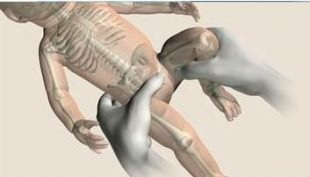
- Barlow test (left) and Ortolani test (right) (see Figure 1)
- When examining hip stabilise pelvis on opposite side
- Can legs be fully abducted
Barlow test (right hip)
- Hip adducted and flexed to 90°
- Hold distal thigh and push posteriorly on hip joint
- Test is positive when the femoral head felt to slide posteriorly as it dislocates
Ortolani test (left hip)
- Stabilise pelvis and examine each hip separately
- In a baby with limited hip abduction in flexion, hip is flexed to 90° and gently abducted while examiner’s finger lifts the greater trochanter
- Test is positive when the femoral head is felt to locate into the acetabulum
Contains public sector information licensed under the Open Government Licence v3.0 https://www.nationalarchives.gov.uk/doc/open-government-licence/version/3/
REFERRAL FOR ENHANCED SCREENING
- Enhanced screening is done through ultrasound of the hips
- NIPE guidelines include specific criteria for referral for enhanced screening and the timescale in which this should occur
- Individual trusts may add local criteria to supplement national criteria
- SCREEN POSITIVE result is an abnormal clinical hip examination (with/without risk factors) or NIPE hip risk factors
Abnormal examination defined as:
- Difference in leg length
- Knees at different levels when hips and knees bilaterally flexed
- Difficulty abducting hip to 90°
- Palpable ‘clunk’ when undertaking Ortolani or Barlow manoeuvre
NIPE hip risk factors:
- Family history of first degree relative with hip problems in early life, unless DDH has definitely been excluded
- Breech presentation at ≥36 completed weeks of pregnancy, irrespective of presentation at delivery or mode of delivery, or
- Breech presentation at the time of birth between 28 weeks’ gestation and term
- In the case of a multiple birth, if any baby falls into either category, all babies in this pregnancy to have ultrasound examination
Additional local criteria for referral may include:
- Significant moulding
- Congenital torticollis, congenital plagiocephaly
- Structural foot deformity
- Congenital calcaneovalgus
- Fixed talipes equinovarus
- Check your local referral criteria
PROCESS
Screen negative − no risk factors on history and normal examination
- No further intervention needed
- Inform parents and document findings
- These babies will be rechecked at their 6–8 week check
Screen positive – (risk factors or abnormal examination as detailed above)
- Inform parents of findings and plan for further investigation
- Document findings and plan
- Request outpatient hip ultrasound to be performed in accordance with NIPE guidance
- For babies born <34+0 weeks’ gestation, hip ultrasound should be undertaken 38−40 weeks’ corrected age
- For babies born ≥34+0, hip ultrasound scan should be undertaken at aged 4−6 weeks
- Departments to have system in place to review all hip scan results and inform parents as they are reported
- babies with normal hip scan require no further action and will be re-examined at their 6–8 week check babies with abnormal hip scan require a specialist assessment
- An outcome decision for all babies should have been made by aged 6 weeks for babies born ≥34+0, and by 40+0 weeks’ corrected age for babies born <34+0 weeks
Dislocated/dislocatable/unstable hip – positive Ortolani or Barlow test or limited hip abduction
- Review by middle grade or consultant to confirm diagnosis
- Inform parents of findings and plan for further investigation and management
- Document findings and plan
- Urgent referral required
- Check local policy regarding referral to physiotherapy/orthopaedic team and ultrasound. Service may be provided locally or referral to a tertiary centre paediatric orthopaedic team may be required
Date updated: 2024-01-17