RECOGNITION AND ASSESSMENT
- Plasma potassium >6 mmol/L (normal 3.0–5.5 lithium heparin specimen)
- Babies often tolerate concentrations up to 7.5–8.0 mmol/L without ECG changes
SYMPTOMS AND SIGNS
- Cardiac arrest
- ECG abnormalities (see below):
- tall peaked T waves
- widened QRS complex
- sine waves (widened QRS complex merging with T wave)
- prolonged PR interval, bradycardia, absent P wave
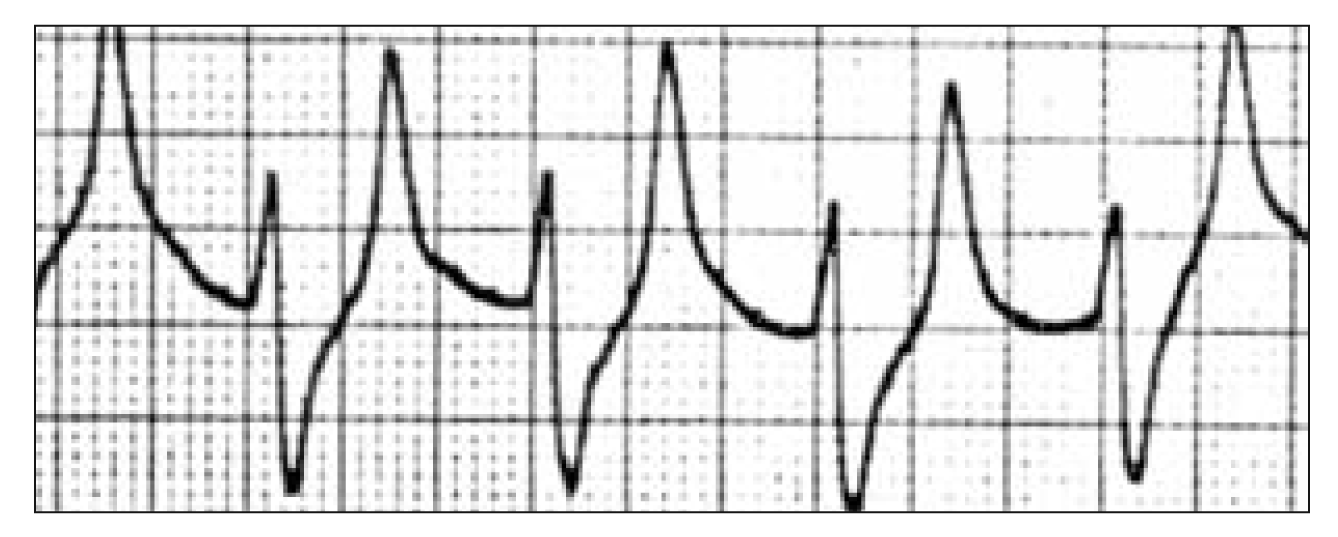
Tall, peaked T wave, widening of QRS
Sine wave QRS complex (before cardiac arrest)
RISK OF ARRHYTHMIA
- ECG changes as above
- Rapid rise in potassium >7 mmol/L
- Ca2+ and Mg2+ below normal range
- Oliguria
- Acute kidney injury
- Known cardiac disease
CAUSES
- Renal failure: secondary to hypoxic ischaemic encephalopathy, sepsis and hypotension, post major surgery, structural abnormalities and nephrotoxic drugs
- Cellular injury with potassium release e.g. large intraventricular haemorrhage, haemolysis
- Very-low-birth-weight babies without renal failure (non-oliguric hyperkalaemia) in first 12–48 hr
- Excess potassium in IV solutions
- Endocrine (congenital adrenal hyperplasia, pseudohypoaldosteronism)
INVESTIGATIONS
- Confirm hyperkalaemia. Send free-flowing venous or arterial laboratory sample to avoid haemolysed sample. Be guided by capillary gas sample in the meantime
- If potassium >6.0 mmol/L, send Ca2+, Mg2+, Cl-, glucose and urinalysis to guide treatment and help identify cause
- If potassium >6.0 mmol/L, commence continuous ECG monitoring and assess for risk of arrhythmia (see above)
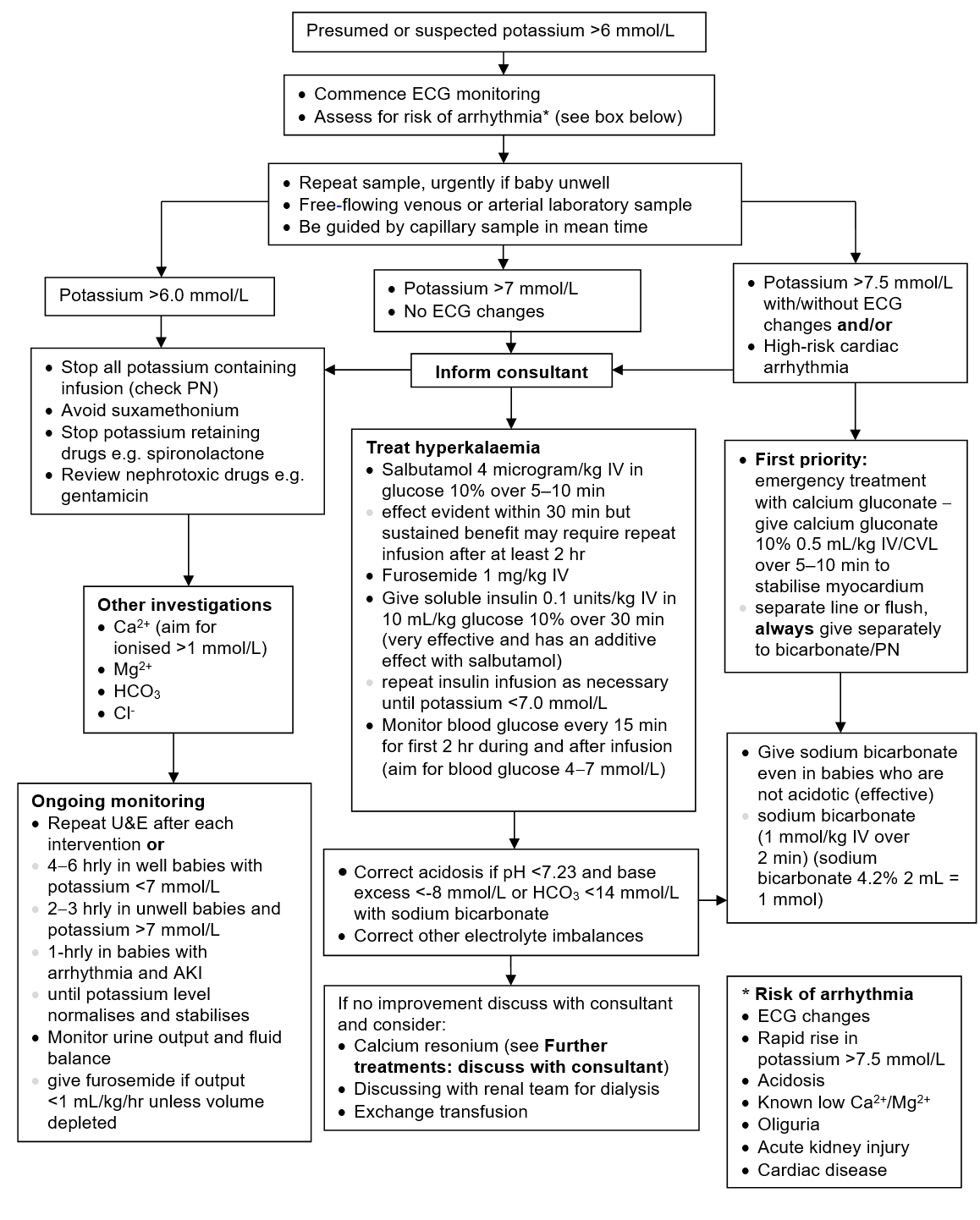
IMMEDIATE TREATMENT
Serum potassium >6.0 mmol/L (stable with normal ECG)
- Stop all sources of potassium including IV solutions (check PN) and oral supplements
- Stop all potassium-retaining drugs and potassium-sparing diuretics e.g. spironolactone
- Avoid suxamethonium
- Review and withhold nephrotoxic drugs e.g. gentamicin
- Recheck U&E 4–6 hrly
Serum potassium >7.0 mmol/L without ECG changes
- As above
- Inform consultant
- Give salbutamol 4 microgram/kg IV in glucose 10% over 5–10 min; effect evident within 30 min but sustained benefit may require repeat infusion after at least 2 hr
- Give furosemide 1 mg/kg IV
- If serum potassium still >7.0 mmol/L, give soluble insulin 0.1 units/kg IV in 10 mL/kg 10% glucose over 30 min; very effective and has an additive effect with salbutamol
- Repeat U&E 2–3 hrly
- Repeat insulin infusion as necessary until potassium <7.0 mmol/L
- Monitor blood glucose every 15 min for first 2 hr during and after infusion
- aim for blood glucose 4.0–7.0 mmol/L
- Give sodium bicarbonate 1 mmol/kg (2 mL of sodium bicarbonate 4.2% = 1 mmol) if:
- pH <7.23 or
- BE more negative than -8 or
- bicarbonate <14 mmol/L
- Correct other electrolyte abnormalities
- Maintain ionised Ca2+ >1 mmol/L
Serum potassium >7.5 mmol/L with ECG changes
- As above, but first institute emergency measures below:
- give calcium gluconate 10% 0.5 mL/kg IV/CVL over 5–10 min
- infuse centrally were possible; does not reduce potassium but stabilises myocardium
- flush line with sodium chloride 0.9% or preferably use a different line
- always give separately to bicarbonate or PN (calcium gluconate must not come into contact with any other IV administered drug)
- give sodium bicarbonate (1 mmol/kg IV over 2 min). Effective even in babies who are not acidotic (2 mL of sodium bicarbonate 4.2% = 1 mmol)
- give calcium gluconate 10% 0.5 mL/kg IV/CVL over 5–10 min
- Repeat U&E hourly
Further treatments: discuss with consultant
- A cation-exchange resin, such as calcium resonium (500 mg/kg rectally, with removal by colonic irrigation after 8–12 hr, repeat every 12 hr. Dose can be doubled at least once to 1 g/kg in severe hyperkalaemia). Useful for sustained reduction in serum potassium but takes many hours to act and is best avoided in sick preterms at risk of necrotising enterocolitis
- If severe hyperkalaemia persists despite above measures in term babies with otherwise good prognosis, contact renal team for consideration of dialysis or exchange transfusion (see Exchange transfusion guideline)
SUBSEQUENT MANAGEMENT
- Recheck serum potassium after each intervention or:
- 4–6 hrly in stable/well baby with potassium <7 mmol/L and no ECG changes
- 2–3 hrly in unwell baby and/or potassium >7 mmol/L with no ECG changes
- hourly when arrhythmias or ECG changes present with/without renal failure
- Monitor urine output and maintain good fluid balance
- If urine output <1 mL/kg/hr, unless baby volume depleted, give furosemide 1 mg/kg IV until volume corrected
- Treat any underlying cause (e.g. renal failure)
- Review need for further investigations for underlying cause e.g. 17OHP for congenital adrenal hyperplasia
Management of hyperkalaemia in babies
Date updated: 2024-02-26