INDICATIONS
- Severely ill baby when immediate vascular access needed, a UVC is not feasible and peripheral access not possible (maximum 2 attempts)
- Cardiac arrest
- allows rapid expansion of circulating volume
- gives time to obtain IV access and facilitates procedure by increasing venous filling
CONTRAINDICATIONS
- Fractures in target bone
- Previous orthopaedic surgery near insertion site
- Previous IO insertion in target bone within the preceding 48 hr
- At insertion site:
- infection
- loss of skin integrity
- inability to locate landmarks or excessive tissue
- Osteogenesis imperfecta (if using a manual Cook needle only)
EQUIPMENT
- EZ-IO drill and needles (3–39 kg: 15 mm pink) or Cook needle
- <3 kg use 18–21 G butterfly needle
- 5 mL syringe with extension and 3-way tap to aspirate and confirm correct position
- 10 mL sodium chloride 0.9% flush
- 20 mL syringe to administer fluid boluses
- Infusion fluid
For manual insertion, infiltrate skin with lidocaine 1% (preservative free) up to 3 mg/kg (0.3 mL/kg) if patient responds to pain
PROCEDURE
Never place your/assistant’s hand under tibia during insertion to avoid staff injury
EZ-IO
- Locate landmarks
- Aseptic non-touch technique: clean site
- If conscious administer local anaesthetic, lidocaine 1% (preservative free) subcutaneously
- Choose short pink hub needle and attach to drill magnetically
- Hold drill and needle at 90° to skin surface and push through skin without drilling, until bone is felt
- Push drill button and drill continuously and push until there is loss of resistance – there is a palpable give as needle breaches the cortex
- Remove drill and unscrew trocar
- If possible aspirate the marrow
- Attach pre-prepared connection tube
- Secure needle (with EZ-IO fixator if available)
- If awake, give lidocaine 1% (preservative free) 0.5 mg/kg (0.05 mL/kg) over 2 min through IO, leave 1 min then flush with sodium chloride 0.9% 2 mL
- Proceed with required therapy
- If EZ-IO drill power fails, repeated clockwise-anticlockwise twisting with gentle pressure allows manual insertion
Cook needle
- Locate landmarks
- Aseptic non-touch technique: clean site
- If conscious administer local anaesthetic, lidocaine 1% (preservative free)
- Stabilise the lower limb laterally, insert needle at 90° to skin surface. Direct needle caudally from the epiphyseal plate at an angle of approximately 60° to the long axis of the tibia
- Advance needle firmly; needle entry into the marrow cavity is accompanied by a loss of resistance, sustained erect posture of the needle without support and free fluid infusion
- Attach 5 mL syringe and confirm correct position by aspirating marrow (may be omitted in patients with circulatory arrest), take any bloods required
- Infuse fluid using 20 mL syringe and IV cannula extension set (with Leur-lock ends)
Preferred site
Avoid fractured bones and limbs with fractures proximal to possible sites
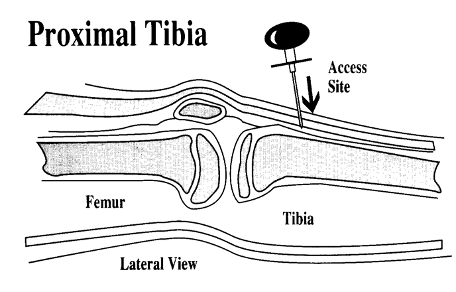
Proximal tibia
- Identify anteromedial surface of tibia approximately 1 cm below tibial tuberosity
- Direct needle away from knee at approximately 90° to long axis of tibia
Access site on proximal tibia – lateral view
COMPLICATIONS
Infrequent (<1%) and include:
- Bleeding
- Infection
- revert to central or peripheral venous access as soon as possible
- Extravasation
- Subperiosteal infusion
- Bone marrow embolism
- Dislodgement
- Skin necrosis
- Compartment syndrome
- observe and measure limb circumference regularly
- palpate distal pulses and assess perfusion distal to IO access site
- Pain from rapid infusion: give lidocaine 1% (preservative free) 0.5 mg/kg (0.05 mL/kg) over 5 min
Date updated: 2024-01-16