INDICATION
- Suspected pneumothorax (e.g. any deterioration in clinical condition, particularly if ventilated)
EQUIPMENT
- Cold light source
- Black drapes to cover incubator
PROCEDURE
-
Dim lights
-
Expose baby’s chest and abdomen
-
Remove all non-essential monitoring leads
-
Cover outside of incubator with black drapes
-
Place cold light tip perpendicular to and touching baby’s skin
-
Shine light from the side, in the 5 positions shown in diagram, comparing right side with left (5th position shines through the liver and is used as a control)
-
Clean cold light tip with an alcohol wipe after use
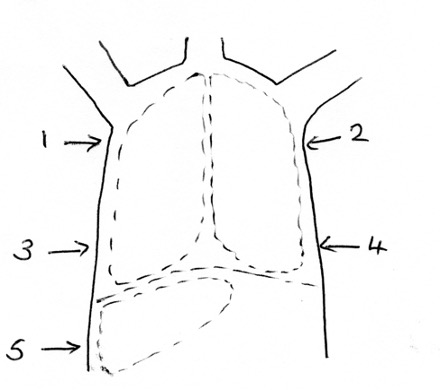
- Right side just below axilla
- Left side just below axilla
- Right side approximately 5th/6th intercostal space
- Left side approximately 5th/6th intercostal space
- Right side just below diaphragm (liver)
DIAGNOSIS
- Pneumothorax confirmed if chest shines bright red
- Compare both sides of chest (babies can have bilateral pneumothoraces)
- Compare degree of brightness with that seen over liver
- liver and lung without pneumothorax will shine dull dark red
Caution - false positive diagnoses may be made in extremely preterm babies and those with pulmonary interstitial emphysema
Transillumination may be unreliable in babies with increased thickness of the chest wall (macrosomic term infants and those with chest wall oedema)
Transillumination may be unreliable in babies with increased thickness of the chest wall (macrosomic term infants and those with chest wall oedema)
ACTION
- If baby is unstable or haemodynamically compromised, once pneumothorax is confirmed on transillumination, perform immediate needle thoracocentesis in 2nd intercostal space, midclavicular line on the side of the chest that shone brightly. Do not wait for a chest X-ray
Date updated: 2024-01-16