Procedure is the same for both nasogastric and orogastric tubes. As nasogastric tubes (NGT) are more commonly used in babies, the term nasogastric will be used throughout this guideline
INDICATIONS
- To keep stomach deflated or to instil enteral feeds when full oral feeding not possible
- Administration of medications when unable to use oral route
- Orogastric tubes are used predominantly in babies in respiratory distress or with structural abnormality of nasal cavity where full bottle feeds are contraindicated
- NGT are used short-term for all other babies until full oral feeding achievable
- An NGT is preferred to an orogastric tube with a few exceptions, such as a structural abnormality (e.g. choanal atresia, cleft lip and palate) and some respiratory distress. It may still be possible to use an NGT if baby receiving nasal mask CPAP, or nasal prong oxygen
EQUIPMENT
- Smallest sized NPSA compliant NGT that will pass: 4 FG, 5 FG or 6 FG to reduce risk of nasal abrasions and ensure baby comfort
- Exceptions – surgical patient in specific clinical circumstances
- Enteral syringe (see https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiv9OmUjpv4AhVFkFwKHTs-C68QFnoECAsQAQ&url=http%3A%2F%2Fwww.premiersafetyinstitute.org%2Fwp-content%2Fuploads%2FOral-medicines-alert.pdf&usg=AOvVaw3PSI2MSRu2c0MpD7lx8Z
- pH testing strips (CE marked for use with human gastric aspirate)
- Extra-thin hydrocolloid dressing (e.g. Duoderm®, Convatec)
- Soft adhesive tape (e.g. Hypafix®, Tegaderm™, Mefix®)
- Non-sterile disposable gloves
PROCEDURE
Preparation
- Discuss procedure with parents/carer
- To prevent risk of aspiration, pass NGT before a feed
- Wash hands and prepare equipment
- Administer sucrose (see Pain assessment and management guideline)
- To reduce risk of epidermal stripping, apply Duoderm® to skin of face as an attachment for adhesive tape
- Determine length of tube to be inserted by measuring nose>ear>mid-umbilicus (NEMU) measurement. Note the cm mark on the tube or keep your fingers on the point measured
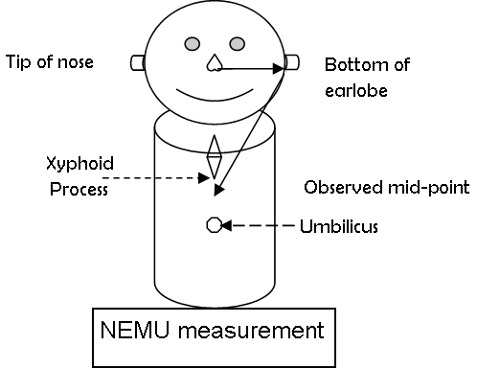
- For orogastric tube, measure as NGT but start from the centre of the bottom lip rather than the nose
Insertion
- With clean hands, put on gloves and pass tube into nose or mouth slowly and steadily until required pre-measured depth reached
- Use of a dummy (with parental permission) may help tube passage
- Observe baby throughout procedure for colour change, vomiting, respiratory distress or resistance
- if any of these features or distress occurs, stop and remove tube and try a different angle or nostril. If resistance felt, abandon procedure – do NOT force the tube
Checking position of nasogastric feeding tube
- NNUs and carers in the community should use pH indicator strips or paper
- Do not use radiography ‛routinely’ but, if baby being X-rayed for another reason, use X-ray to confirm position is satisfactory by noting position of tube on film
- Do not use ‛Whoosh test’ (auscultation of injected air entering the stomach) to determine position of NGT as it is unreliable
Checking position using pH
- Aspirate stomach contents with enteral syringe and test for acid response using pH testing strips
- pH ≤5.5 indicates correct gastric placement. If pH 5 or 5.5, confirm pH interpretation with a second person before commencing feed
- if pH ≥6, do not commence feed. Repeat aspiration and retest
- if repeated test ≥6, seek advice from senior clinician and undertake risk assessment
- Following factors can contribute to high gastric pH ≥6
- presence of amniotic fluid in baby <48 hr
- milk in baby’s stomach, particularly if 1–2 hrly feeds
- use of medication to reduce stomach acid
- tube positioned in jejunum or duodenum
- tube positioned in lungs
- Multidisciplinary care team to then discuss possible actions, balancing risk of feeding (with possibility of tube being in the lungs) and not feeding baby in the short-term, and record how decision reached
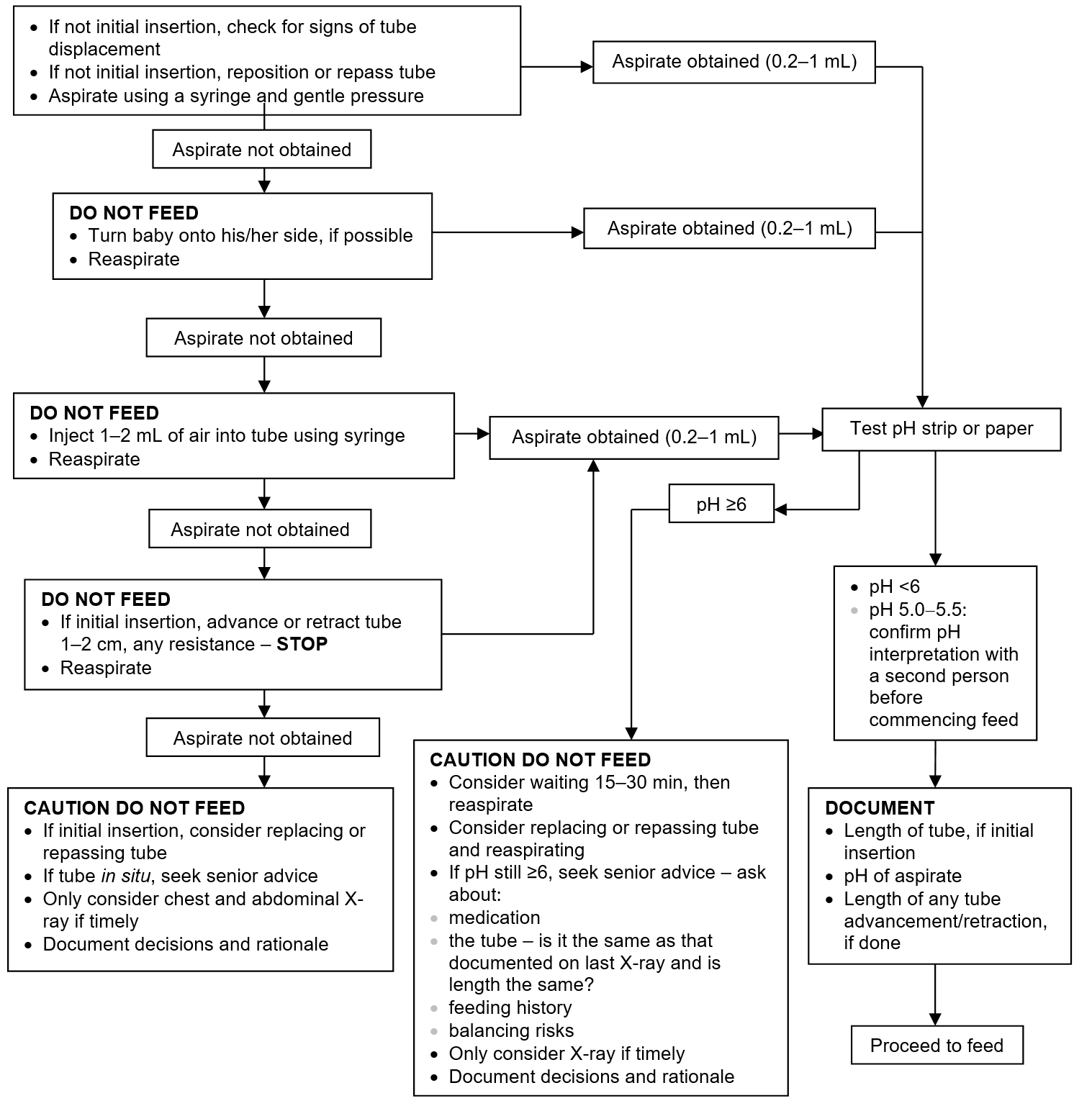
- Ensure you work through NPSA flowchart and record findings before making any decisions
NPSA flowchart: A basis for decision-making when checking position of naso- and orogastric feeding tube in babies on NNU
Securing tube
- Once correct tube position ascertained, secure to face with soft adhesive tape (e.g. Hypafix® or Mefix®) over Duoderm®
FURHTER MANAGEMENT
Monitoring
-
Check integrity of skin around nostril at frequent intervals for signs of deterioration
-
if signs of pressure appear, reposition tube and/or tape, or repass NGT via opposite nostril, or use orogastric route if necessary
-
-
Check NGT position by measuring pH of aspirate. Follow NPSA flowchart:
-
after initial insertion and subsequent reinsertions
-
before administering each feed
-
before giving medication
-
after vomiting, retching or coughing (absence of coughing does not rule out misplacement or migration)
-
if evidence of tube displacement (e.g. if tape loose or visible tube appears longer or kinked)
-
when chest X-ray taken for another reason
-
-
If receiving continuous feeds, use appropriate giving set and check pH when changing set
-
when continuous feeding has stopped, wait 15–30 min to allow stomach to empty of milk and for aspirate pH to fall
-
Changing NGT
- Follow manufacturer’s recommendations
- Ensure safe and gentle removal of tape using water, applied with cotton bud to soften adhesive tape. Never be tempted to rip tape directly from the skin
- Pass new NGT via opposite nostril wherever possible
- Document removal/replacement in baby’s medical record
Reporting misplaced tube incidents
- Report all misplaced feeding tube incidents using local risk management procedure
FURTHER INFORMATION
- Further details on determining correct position of oro-/nasogastric tubes in babies available from https://www.england.nhs.uk/wp-content/uploads/2016/07/Resource_set_-_Initial_placement_checks_for_NG_tubes_1.pdf